
Cruel and unnecessary punishment: Asylum seekers will foot half of department’s cost-cutting blitz

Fast facts:
The federal government is seeking $60 billion in spending cuts to pay for the doubling of the Department of National Defence budget. New information has come to light revealing asylum seekers will be among the first to pay the price.
- Almost half of Department of Immigration, Refugees and Citizenship Canada (IRCC) cuts will come from a single cut in health care coverage for asylum seekers.
- They’ll face a 30 per cent cut in dental care support and a new prescription drug co-payment.
- That’s a quarter billion dollars’ worth of health care cuts.
- Asylum seekers come to Canada with little to nothing, since they’re escaping dangerous conditions. Most won’t be able to pay the extra costs and will simply avoid dental care and filling prescriptions—until an emergency arises.
- They’ll end up in Canada’s emergency rooms, which will also be paid by IRCC, but at 100 per cent of the cost, even though prevention is preferable and less expensive than the emergency room.
You can’t cut $60 billion in programs and avoid service level impacts. Asylum seekers’ health care is our first peek at what these major cuts will mean. We’ll pay more in the long run, asylum seekers will endure unnecessary suffering, and the Department of National Defence will keep swelling in size.
Cutting health care for asylum seekers
The federal government’s 2025 budget introduced a massive $60 billion in cuts over the next five years. These cuts, now called the “Comprehensive Expenditure Review” (CER) were rushed through, with departments developing detailed plans in only a few months last summer. Those cuts will effectively pay for doubling the budget for the Department of National Defence.
The budget promised that “savings will be achieved by restructuring operations and consolidating internal services and rightsizing programs to realise efficiencies.” Now we’re seeing the first signs that nothing could be further from the truth. Initial hints are that these cuts will come at direct impact on tangible services—forget efficiencies.
On February 12, the Parliamentary Budget Office released a costing exercise on the Interim Federal Health Program, a program meant to provide basic health care coverage for asylum seekers. Buried in a footnote of that report, we’ve actually gained a major insight into how Immigration, Refugees and Citizenship Canada (IRCC) plans to hit its CER cuts goal.
Almost half of IRCC cuts will come from a single cut in health care coverage for asylum seekers. This has nothing to do with efficiencies or AI or the IRCC’s stated goals of “rationalizing programming, while upholding the government’s long-standing commitment to resettle the world’s most vulnerable.” It’s a straight up public service cut to health care provision for Canada’s most vulnerable.
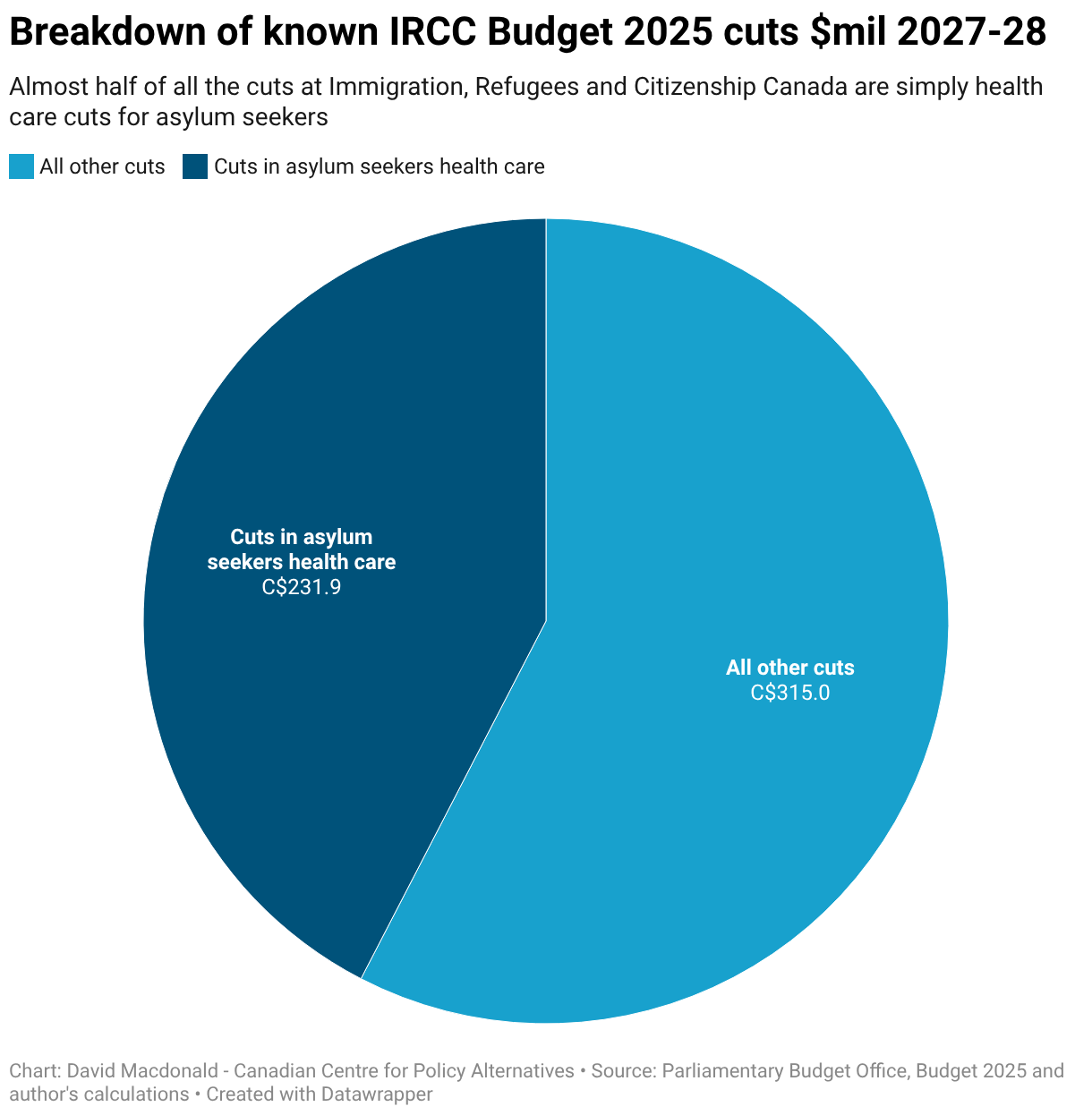
Specifically, IRCC plans to make asylum seekers pay more for prescription drugs and also cover 30 per cent of expenses like dental care. This is what will represent roughly half of the cuts IRCC plans to implement. There also seems to be an assumption that asylum seekers, some of the most vulnerable people in Canada, will pick up this quarter-billion-dollar tab. In reality, what they’ll likely do is avoid treatment for dental issues and avoid filling prescriptions.
The shocking part about this “plan” is that, while IRCC is levying higher costs for preventative treatments like prescriptions and dental care on asylum seekers, it will still cover 100 per cent of the costs to go to emergency rooms or to visit a physician. This is a bizarre accounting exercise where you “save” money through co-pays but the costs add up on the emergency health care side of the equation, which IRCC also pays for.
Asylum seekers are less likely to have workplace insurance for dental or prescriptions. These expenses are all out of pocket for them. They are likely working at low-paying jobs, if they have a work permit. They’ll likely be unable to cover these expenses. And the types of jobs asylum seekers are likely to obtain aren’t the sort that will offer comprehensive health insurance benefits.
Ironically, one of the justifications for our new national Canadian Dental Care Plan was that lower-income families avoid dental visits due to their high cost and they shouldn’t be. Oral health problems are particularly prevalent among refugee child populations. And tooth infections are the most common childhood day surgery in Canada. While Canadian families making under $90,000 are now covered by the national plan, asylum seekers won’t be, starting May 1, and will have to pay a third of the cost out of pocket.
The Hoskins report on pharmacare notes that millions of Canadians struggle to afford prescriptions due to co-payments—the type of co-payments we’ll now be forcing on asylum seekers. The direct result of co-payments is that people don’t fill prescriptions and take much needed drugs. The downstream impact of not taking meds for diabetes, cardiovascular disease and chronic respiratory conditions alone led to a quarter of a million unnecessary emergency visits for Canadians. Something that will become much more common for asylum seekers.
To date, asylum seekers’ health care cuts are the only costed service impact we have from IRCC, but the department also promised to cut housing benefits for asylum seekers and settlement programs for economic immigrants. If, and when, the value of those cuts is revealed, it may become very clear that service cuts are what the CER is all about.
At IRCC, it’s pretty clear that the cuts starting in May are levied against Canada’s most vulnerable in a way that will surely drive many to the emergency room—ultimately driving up governments’ health care costs because it’s more expensive to deal with a problem in emergency than it is to prevent it in the first place. That’s called the social determinants of health and the government should be making evidence-based decision-making to help everyone in Canada prevent health care problems, rather than cut budgets that will only worsen health outcomes.
These initial hints at service level impacts set an ominous tone for what the CER cuts will look like in other departments.
A cut in one place will inevitably lead to costs elsewhere. In this case, the department is burdening asylum seekers in the short-term, but will run up costs in the health care system over the long term—costs, incidentally, that are also IRCC’s.
link





